Comeback to Covid-19 disease – what to consider?
von
Gastautor
Gepostet am 11.3.2022
For 2 years, the Corona Pandemie has now influenced amateur and professional football, alongside social and economic life. With the beginning of the pandemic, sports physicians and scientists investigate the question of how athletes after a corona disease can optimally return to sports activity and ultimately to competition without a health risk arising. In the following article, you will find out what to consider for footballers after a Covid-19 infection when returning to sports and how an individually coordinated stress build-up can take place.
What effect can a Covid-19 infection have on footballers?
Footballers and footballers are exposed to high loads during sporting activity. Covid-19 can cause acute damage to the heart muscle and chronic damage in the cardiovascular system (Zheng et al., 2020, p.259). If after a Covid-19 infection is too fast and too high, this can lead to cardiac muscle inflammation, which can also threaten long-term damage. Therefore, the return-to-sport issue for a Covid-19 infection is enormously important in order to be able to rule out the risk of cardiac damage (e.g. myocardialitis) or pulmonary involvement (Kriemler et al., 2021, p.9). In order to avoid this Worst-Case scenario, targeted medical diagnostics as well as an individually adapted load build-up after Covid-19 infection in power and amateur football are absolutely necessary.
When can footballers return to training after Covid-19 infection?
In order to make the re-entry of footballers optimal after a Covid-19 infection, an assessment of the course of the disease is necessary (Kriemler et al., 2021, p.2). The extent of the medical diagnosis carried out depends on the clinical course of the infection (Burgstahler & Nieß, 2021, p.249). The return-to-sport algorithm as well as the extent of the diagnostic measures according to a Covid-19 disease of the DGSP (German Society for Sports Medicine and Prevention) and the VGB (Administrative Professional Cooperative).
Table 1: Return-to-Sport algorithm according to Covid-19 disease of DGSP and VGB (Burgstahler & Nieß, 2021, p.251; Nieß et al., 2020; VGB, 2021)

In principle, athletes do not belong to the risk groups of a Covid-19 infection (Nieß et al., 2020, p.1). They even have better conditions to deal with an infection, as sports activity strengthens the immune system (Lancaster & Febbraio, 2016, p.115). Most of the infections are asymptomatic in young athletes or with slight symptoms (Kriemler et al., 2021, p.9). Severe courses in sportsmen are rare, but still occur (Nieß et al., 2020, p.1).
What to consider when returning to sports activity?
In any case, consultation with a doctor (e.g. general physician, cardiologist or sports physician) should first be held. If all of the diagnostic measures taken have been inconspicuous and the sports carence has been strictly adhered to as a function of the course of the disease, a step-by-step stress can finally be established. Above all, the fitness condition of the athlete, which had existed before the infection, should serve as an anchor point. This primarily specifies the goal that can be achieved during the setup training to be able to participate again in the competition events. Should the fitness condition of the athlete have been adversely affected before the Covid-19 infection (e.g. due to a different injury), this must be taken into account in building training.
Example plan of a step-by-step stress build-up after asymptomatic or slight disease course (modified according to VGB, 2021)
Phase 1
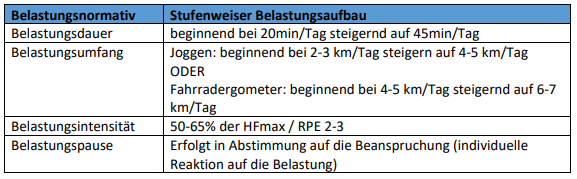
In the first 2-4 days of training, the athlete is first used to the load. Possible training contents that can be carried out are mobilization exercises, bicycle ergometers or light jogging (duration method). The aim of this phase is to increase the load duration and the load range at low load intensity.
Table 2: Example plan Training Control Phase 1
If the athlete does not show any special vulnerabilities in this phase during or after the load, it can be converted to phase 2.
Phase 2
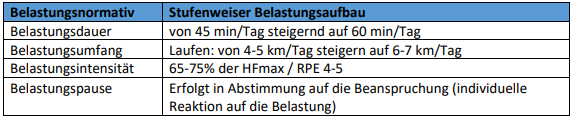
During the 2nd phase, the load duration, the load extent and the load intensity are further increased in the following 2-3 days. Possible training contents during this phase are mobilization and stabilization exercises, co-ordinative exercises and running ABC as well as simple technical exercises with ball (e.g. pass and dribbling forms) and endurance courses (continuous method, extensive intervals).
Table 3 Example plan Training Control Phase 2
If the athlete does not show any special vulnerabilities in this phase during or after the load, it can be converted to phase 3.
Phase 3
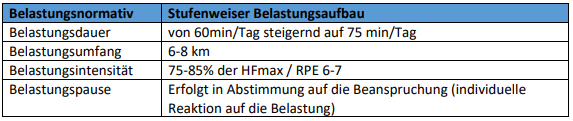
In the third phase (2-4 days), the load duration is further slightly increased. The main focus in this phase is the increase in the load intensity. Possible training contents in this phase are: mobilization, stabilization and strengthening exercises, running ABC, football-specific motion patterns (stop and go, change of direction), ball work (passion: short/long/flight balls, dribbling, gate closures) and increase and endurance courses (extensive and intensive intervals).
Table 4: Example Plan Training Control Phase 3
If the athlete does not show any special vulnerabilities in this phase during or after the load, it can be converted to phase 4.
Phase 4
During the 4th phase (2-4 days), the builder is partially integrated into the team training. Submaximum exercise and play forms are possible as a wall player or neutral player.
Table 5: Example plan Training Control Phase 4
If the athlete does not show any special vulnerabilities in this phase during or after the load, he/she can enter the team training again.
Notes:
The monitoring takes place in all phases via tracking of the live heart rate as well as via the interrogation of the subjective stress sensation (RPE).
If the athlete shows vulnerabilities during or after the load (e.g. dizziness, short breathing, cardiac turf or circulatory problems) the load is immediately to stop to consult a doctor.
Construction training after Covid-19 infection with severe illness should be carried out under medical consultation and medical control.
Conclusion
The main information is summarized below:
- every athlete should be individually assessed after recovery
- the guidelines for an optimal return to sports are based on the severity of the disease after a corona infection (Kriemler et al., 2021, p.2)
- the fitness condition of the athlete before the infection should be included in the evaluation and planning of the training
- the load build-up takes place stepwise after exposure
- monitoring the live heart rate and direct feedback (assessment RPE, questions about vulnerabilities during or after the load) of the athletes during the setup training units serve to assess the stress and thus to further load control
Attention:
The Return-to-Sport guidelines after a Covid-19 infection are constantly being adapted and can vary according to the state, treating physician and current state of science.
In the event of a doubt, ‘Safty First, instead of false ambition’ and prefer to make a few days longer. Because our health is, in addition to our lifetime, the most important thing that we possess people.
Liability Committee
The author and the company SportSense are not responsible for the topicality, correctness and completeness of the information provided. Liability claims against the author or SportSense, which relate to damages of a material or ideological nature caused by the use or non-use of the information provided or by the use of incorrect and incomplete information, are excluded, provided that the author or SportSense has not proven to have caused them intentionally or grossly negligently.
If you want to see more interesting posts from us, follow us on Facebook: Click here!
Or come in our Facebook group "Modern Football Training - Focus on Athletics" and discuss with us and other trainers about exciting topics: Click here!
About the author Andreas Kellner

M. Sc. Sports Scientist
Athletics trainer Hertha BSC Berlin U16
UEFA Trainer Level-B
Fitness trainer A-Licence
Contact: andreas.kellner@herthabsc.de
Instagram: andreas.kllnr
Literature
Burgstahler, C., & Nieß, A. M. (2021). Return to Sports after COVID-19. Sports Orthopaedics and Traumatology, 37(3), 249-254.
Kriemler S., Siaplaouras, J., Förster, H., Joisten, C. COVID-19 for young athletes: diagnosis and return to sports. Swiss journal of sports medicine & sports traumatology 69.3.
Lancaster, G. I., & Febbraio, M. A. (2016). Exercise and the immune system: implications for elite athletes and the general population. Immunology and cell biology, 94(2), 115-116.
Nieß, A. M., Bloch, W., Friedmann-Betten, B., Grim, C., Halle, M., Hirschmüller, A., ... & Mayer, F. (2020). Position: return to sport in the current coronavirus pandemic. Dtsch Z Sportmed, 71, E1-4.
VGB (2021). Industry-specific action aid for the SARS-CoV-2 standard for the sports company sector - return to sport after COVID-19. Access to 02.08.2022 at https://www.vbg.de/DE/3_Praevention_and_Working aids/3_Actual_and_Seminare/6_Actuals/Coronavir us/Brancheninfos_Working protection standard/Sport clubs_Rueckkehr_nach_COVID_19.92;jsessionid=015254C49 63C28A3
Zheng, Y. Y., Ma, Y. T., Zhang, J. Y., & COVID, X. X. (2020). COVID-19 and the cardiovascular system Nat. Rev. Cardiol, 17(5), 259-260.